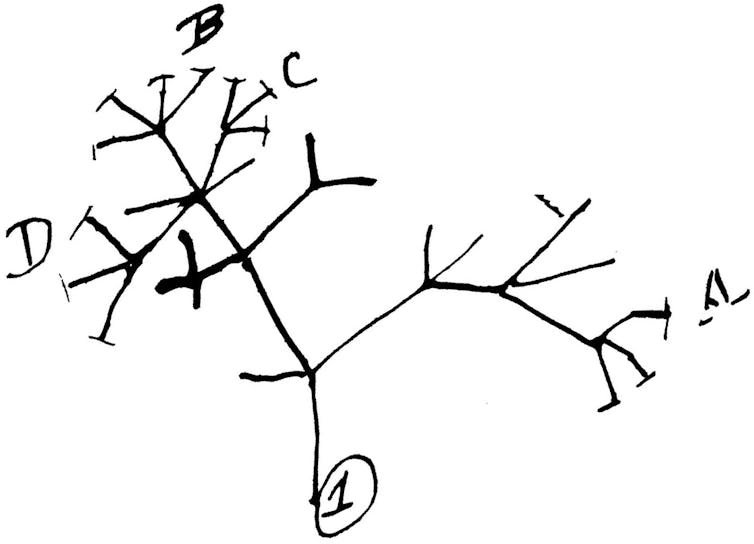
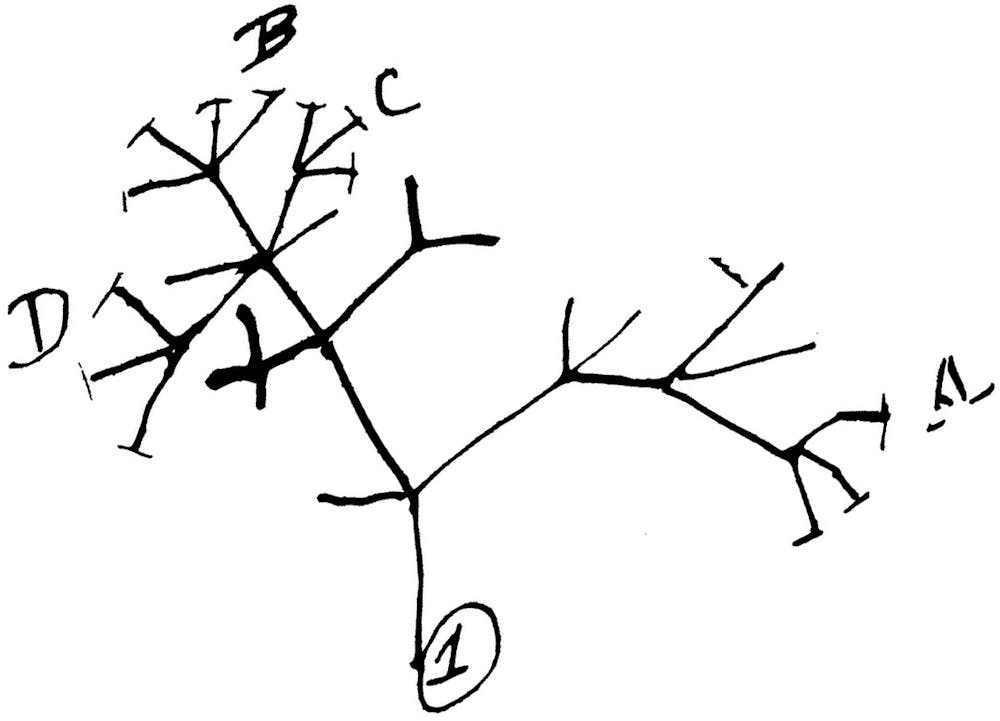
When you hear the term “evolutionary tree,” you may think of Charles Darwin and the study of the relationships between different species over the span of millions of years.
While the concept of an “evolutionary tree” originated in Darwin’s “On the Origin of Species,” one can apply this concept to anything that evolves, including viruses. Scientists can study the evolution of SARS-CoV-2 to learn more about how the genes of the virus function. It is also useful to make inferences about the spread of the virus around the world, and what type of vaccine may be most effective.
I am a bioinformatician who studies the relationships between epidemics and viral evolution, and I am among the many researchers now studying the evolution of SARS-CoV-2 because it can help researchers and public health officials track the spread of the virus over time. What we are finding is that the SARS-CoV-2 virus appears to be mutating more slowly than the seasonal flu which may allow scientists to develop a vaccine.
Charles Darwin’s first diagram of an evolutionary tree, drawn in 1837.Cambridge University Library
How do sequences evolve?
Viruses evolve by mutating. That is, there are changes in their genetic code over time. The way it happens is a little like that game of telephone. Amy is the first player, and her word is “CAT.” She whispers her word to Ben, who accidentally hears “MAT.” Ben whispers his word to Carlos, who hears “MAD.” As the game of telephone goes on, the word will transform further and further away from its original form.
We can think of a biological genetic material as a sequence of letters, and over time, sequences mutate: The letters of the sequence can change. Scientists have developed various models of sequence evolution to help them study how mutations occur over time.
Much like our game of telephone, the genome sequence of the SARS-CoV-2 virus changes over time: Mutations occur randomly, and any changes that occur in a given virus will be inherited by all copies of the next generation. Then, much as we could try to decode how “CAT” became “MAD,” scientists can use models on genetic evolution to try to determine the most likely evolutionary history of the virus.
How can we apply this to viruses like COVID-19?
DNA sequencing is the process of experimentally finding the sequence of nucleotides (A, C, G and T) – the chemical building blocks of genes – of a piece of DNA. DNA sequencing is largely used to study human diseases and genetics, but in recent years, sequencing has become a routine part of viral point of care, and as sequencing becomes cheaper and cheaper, viral sequencing will become even more frequent as time progresses.
RNA is a molecule similar to DNA, and it is essentially a temporary copy of a short segment of DNA. Specifically, in the central dogma of biology, DNA is transcribed into RNA. SARS-CoV-2 is an RNA virus, meaning our DNA sequencing technologies cannot directly decode its sequence. However, scientists can first reverse transcribe the RNA of the virus into complementary DNA (or cDNA), which can then be sequenced.
Given a collection of viral genome sequences, we can use our models of sequence evolution to predict the virus’s history, and we can use this to answer questions like, “How fast do mutations occur?” or “Where in the genome do mutations occur?” Knowing which genes are mutating frequently can be useful in drug design.
Tracking how viruses have changed in a location can also answer questions like, “How many separate outbreaks exist in my community?” This type of information can help public health officials contain the spread of the virus.
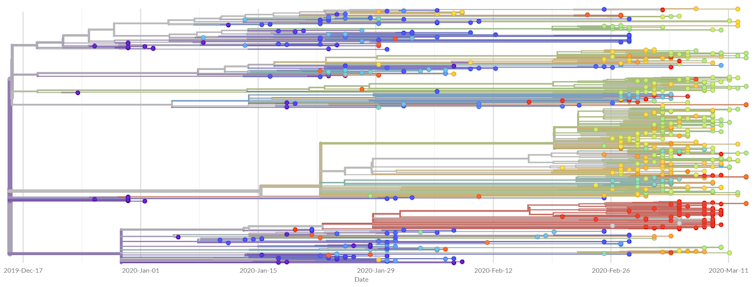
One such initiative is Nextstrain, an open-source project that provides users real-time reports of the spread of seasonal influenza, Ebola and many other infectious diseases. Most recently, it has been spearheading the evolutionary tracking of COVID-19 by providing a real-time analysis as well as a situation report meant to be readable by the general public. Further, the project enables the global population to benefit from its efforts by translating the situation report to many other languages.
As the amount of available information grows, scientists need faster tools to be able to crunch the numbers. My lab at UC San Diego, in collaboration with the System Energy Efficiency (SEE) Lab led by Professor Tajana Šimunić Rosing, is working to create new algorithms, software tools and computer hardware to make the real-time analysis of the COVID-19 epidemic more feasible.
Evolutionary tree of COVID-19 genomes inferred by Nextstrain.from nextstrain.org/ncov
What have we learned about the epidemic?
Based on current data, it seems as though SARS-CoV-2 mutates much more slowly than the seasonal flu. Specifically, SARS-CoV-2 seems to have a mutation rate of less than 25 mutations per year, whereas the seasonal flu has a mutation rate of almost 50 mutations per year.
Given that the SARS-CoV-2 genome is almost twice as large as the seasonal flu genome, it seems as though the seasonal flu mutates roughly four times as fast as SARS-CoV-2. The fact that the seasonal flu mutates so quickly is precisely why it is able to evade our vaccines, so the significantly slower mutation rate of SARS-CoV-2 gives us hope for the potential development of effective long-lasting vaccines against the virus.
The race is on to find a drug that is both effective and safe for treating COVID-19, which has spread to 3.1 million infections and caused 220,000 deaths worldwide.
This week, the US National Institute of Allergy and Infectious Diseases released findings of a clinical trial of the experimental antiviral drug remdesivir. This showed COVID-19 patients recovered more quickly and had an improved survival rate when taking the drug, compared with those given a placebo and standard care.
But these are just the preliminary results of one study. Other human trials have not shown similar results. Further trials are under way and will more definitively show whether remdesivir is a suitable and effective treatment for COVID-19.
What is remdesivir?
Remdesivir is an experimental antiviral drug being developed by Gilead Sciences. Originally it was being developed as a treatment for Ebola, a viral infection that causes severe internal bleeding. But researchers are now interested in its potential to treat patients with COVID-19.
Remdesivir mimics a natural ingredient called adenosine of DNA and RNA, the latter being a molecule similar to DNA that is used to carry the genetic information of viruses. After the drug is activated in the body, it works by blocking a type of enzyme called a polymerase, which is needed to make DNA and RNA.
When you block the enzyme, the virus can’t make copies of itself, limiting the development of symptoms and spread of the disease.
It should be noted that no drug is perfectly safe, and remdesivir is no different. Studies undertaken so far suggest the drug may damage the liver and cause other short-term side effects such as nausea and vomiting.
These side effects need to be taken into consideration when treating COVID-19 patients who have other underlying conditions.
Clinical trials in US positive but only preliminary
This week the National Institute of Allergy and Infectious Diseases (NIAID) released the results of its trial using remdesivir for COVID-19 patients. They studied the effects of the drug on patients who were already infected with COVID-19 to see whether it helped them recover faster and improve their survival rate.
Adult patients hospitalised with COVID-19 were given daily injections of remdesivir. They were found to recover four days faster, an improvement of 31%, when compared with other patients who only received standard care and placebo.
The results also indicated that more patients survived the infection with remdesivir treatment, with the death rate dropping from 11.6% to 8%.
The results are significant enough that director of NIAID Anthony Fauci said it was an “ethical responsibility” for the remaining trial patients who were taking the placebo to be switched to the active drug.
But we need to treat the results of this trial with caution; for the moment they are only preliminary. Read More: masks for COVID-19
A data and safety panel has looked at the initial results, but they haven’t been peer-reviewed. During peer review, independent experts from the scientific community scrutinise the study design, methods, data produced, and the conclusions before the study is published in a medical journal.
How does it compare with other studies?
The results of other trials, such as one undertaken in China, have not shown the same promising results.
The Chinese study was published in the Lancet, considered one of the most influential medical journals in the world. This trial was a randomised, double-blind, placebo-controlled study which means that neither the researchers nor the patients knew if they’d been given the active drug or a placebo.
These types of studies can reduce some biases that can influence studies, but also help quantify the effectiveness of the drug.
But the study also had limitations that need to be recognised. The patients were not as seriously ill as those in the NIAID trial, and the study was terminated early because the outbreak in China was easing.
In the end, the study only collected data on 237 patients, compared with 1,063 patients in the NIAID trial. The authors acknowledge further study is needed in more seriously ill patients and with a larger sample size.
Currently there are more than a dozen other clinical trials of remdesivir and COVID-19 being undertaken throughout the world. We need to await the data to know for sure whether the drug is as effective as we need it to be.